

In clinical psychology, one of the more counterintuitive patterns that emerges when working with high-performing women is this: the higher the level of competence, the more acute the experience of self-doubt.
This is a mechanism. And once you understand the mechanism, the experience of impostor syndrome shifts from something that happens to you into something that tells you something useful.
Impostor syndrome was first documented in 1978 by psychologists Dr. Pauline Rose Clance and Dr. Suzanne Imes, who observed it specifically in high-achieving women who, despite external evidence of their competence, attributed their success to luck, timing, or deception rather than ability. The phenomenon has since been documented across genders and industries, with research published in the International Journal of Behavioral Science estimating it affects approximately 70% of high achievers at some point in their careers.
The conventional approach to impostor syndrome is to treat it as a problem: identify it, challenge it, overcome it. That framing is not only incomplete. It actively works against the people it is supposed to help. Ηowever, I am here to state a different position. Impostor syndrome is not a flaw in your psychology. It is a signal in your system, and learning to read it is more useful than learning to suppress it.
The Neuroscience of Self-Doubt: Why High Achievers Experience Impostor Syndrome More, Not Less
Understanding why impostor syndrome intensifies with success requires a brief look at how the brain processes competence and threat simultaneously.
The prefrontal cortex, responsible for rational evaluation and self-assessment, does not operate in isolation. It is in constant dialogue with the amygdala, the brain's threat-detection system. When you enter a high-stakes situation, whether it’s a board presentation, a salary negotiation, a promotion panel, the amygdala registers the social and professional risk involved. It does not distinguish between physical danger and social evaluation. Both trigger the same threat response.
For high achievers, the amygdala activation is often proportional to how much the outcome matters. The higher the stakes you have set for yourself, the more aggressively your threat system monitors for potential failure. Don’t assume that this is a dysfunction; it’s actually your brain accurately registering that something important is at risk.
The cognitive distortion that follows — the "I don't belong here" or "they will find out I don't know what I'm doing" narrative — is the amygdala's threat response being interpreted by the brain's verbal centers, and it is not an accurate assessment of your competence. It is fear producing a story.
The distinction matters because the standard advice for impostor syndrome — "challenge your negative thoughts" — attempts to fight the amygdala with the prefrontal cortex. This is not a reliable strategy. You cannot reason your way out of a threat response mid-activation. What you can do is learn to recognize the physiological state for what it is, and separate the signal (this matters to me) from the story (therefore, I am fraudulent).
The Clance-Imes Cycle: How Impostor Syndrome Perpetuates Itself
Dr. Clance documented a self-reinforcing cycle that explains why impostor syndrome does not resolve on its own, even after repeated success. The cycle has four stages:

A new achievement or challenge triggers anxiety and fear of failure.
The individual responds with either over-preparation (working excessively to ensure success) or procrastination (avoiding the task to delay potential failure).
Success is achieved. But instead of updating the self-concept to include this evidence of competence, the individual attributes the success to effort ("I just worked harder than everyone else") or luck ("it went well this time").
Because the internal narrative has not updated, the next challenge triggers the same cycle with equal or greater intensity.
This is why impostor syndrome does not simply go away with more achievement. The mechanism that processes success is broken in a specific way: it accepts failure as evidence of incompetence but refuses to accept success as evidence of competence. Addressing impostor syndrome requires directly targeting this asymmetry.
Reframing Impostor Syndrome: From Psychological Liability to Performance Signal
The reframe this article proposes is not motivational. It is structural. Impostor syndrome, read correctly, contains two pieces of useful information.
Signal One: You Are Operating at the Edge of Your Current Capability
Impostor syndrome is, by definition, absent in contexts where you are fully comfortable. You do not experience it when doing tasks you have mastered. You experience it when you operate in territory that extends beyond your current confirmed capability.
This is precisely where professional growth occurs. If you are consistently free of self-doubt in your work, you are not challenged enough. The presence of impostor syndrome is a reliable indicator that you are working at the right difficulty level — the zone where learning and performance development actually happen.
This does not make the experience comfortable. It does make it diagnostic. When the self-doubt activates, the question to ask is not "am I good enough for this?" but "what specifically do I need to close the competence gap I am sensing?"
Signal Two: The Stakes Are Proportional to Your Standards
Impostor syndrome is almost entirely absent in people who do not care about the quality of their work. It is overwhelmingly concentrated in people who do. The anxiety you feel before a high-stakes presentation is not evidence that you will fail. It is evidence that you care about doing it well.
The clinical term for this is performance anxiety, and at moderate levels, it is associated with improved outcomes, not worse ones. The Yerkes-Dodson curve, one of the most replicated findings in performance psychology, demonstrates that performance improves with arousal up to an optimal point, then declines. Moderate anxiety is on the right side of that curve. It sharpens attention, increases preparation, and narrows focus.
The problem is not the anxiety but the narrative that the anxiety generates. Separating the physiological state from the interpretive story it produces is the core skill that distinguishes people who use impostor syndrome as fuel from people who are paralyzed by it.
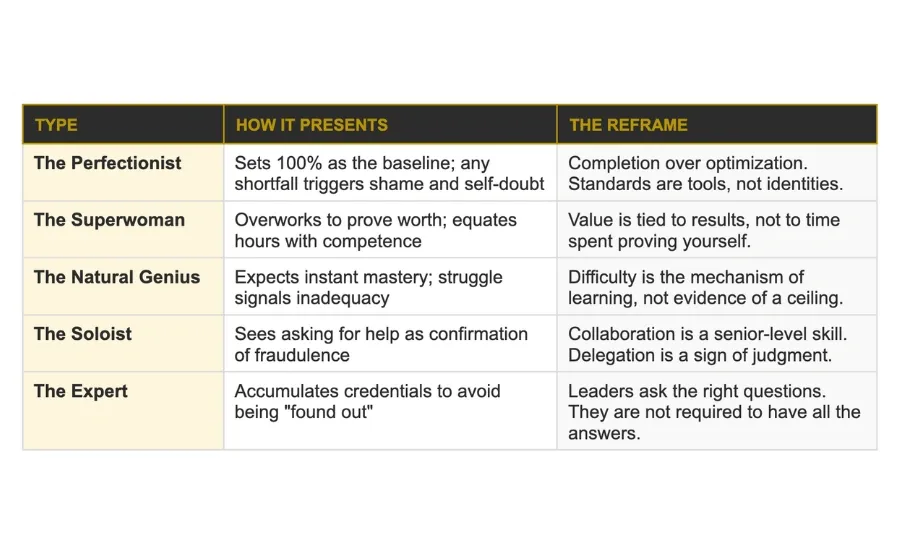
The Five Types of Impostor Syndrome: Identifying Your Specific Pattern
Dr. Valerie Young's research identifies five distinct presentations of impostor syndrome, each with a different internal logic and a different strategic response. Identifying which pattern you operate in is more useful than applying generic advice.
Most people recognize themselves in more than one type. The dominant pattern is usually the one that activates most frequently under pressure.
The Evidence File: A Cognitive Tool for Interrupting the Impostor Cycle
The most effective behavioral intervention for impostor syndrome targets the asymmetric processing described above: the tendency to discount success while accepting failure as confirmation. The Evidence File is a structured method for creating a factual counterweight to the impostor narrative.
How to Build and Use an Evidence File
An Evidence File is a maintained document, digital or physical, that records specific, factual evidence of competence. Not general confidence statements. Not affirmations. Documented facts.
What belongs in it:
Specific accomplishments with measurable outcomes ("delivered X project three weeks early with no scope reduction")
Positive feedback in original form: copied emails, performance review excerpts, direct quotes from stakeholders
Skills acquired and demonstrated in real contexts, not just credentials held
Situations where you were uncertain and succeeded anyway. These are particularly valuable because they directly contradict the core impostor belief
How to use it:
When the impostor narrative activates, before a high-stakes meeting, during a period of self-doubt, after a mistake that feels disproportionately large, open the file and read three entries. The goal is not to feel better. The goal is to introduce accurate data into a cognitive process that is currently operating only on distorted data.
The brain's threat response is not amenable to direct argument. It responds to repetition and specificity. Reading the same concrete evidence repeatedly, over time, begins to update the internal narrative in a way that telling yourself "you are capable" does not.
Impostor Syndrome and Burnout: The Connection Most Frameworks Miss
Impostor syndrome and burnout are rarely discussed together, but they share a direct causal relationship that is worth naming explicitly.
The two primary behavioral responses to impostor syndrome — over-preparation and the inability to delegate — are both significant burnout accelerators. The Superwoman type, in particular, operates on the premise that working more is the only acceptable proof of competence. This produces a pattern where rest, recovery, and appropriate workload boundaries become psychologically impossible because they feel like admissions of inadequacy.
Over time, the sustained activation of the threat response consumes the cognitive and emotional resources required for the kind of high-level, creative work that actually builds competence. Impostor syndrome left unaddressed does not just cause distress. It actively degrades the performance it is trying to protect.
Recognizing this connection is important for two reasons. First, it means that managing impostor syndrome is not a therapeutic nicety. It is a professional performance intervention. Second, it provides a concrete, practical rationale for the behaviors that impostor syndrome makes feel dangerous: rest, delegation, acknowledging limits, asking for support. These are not concessions to inadequacy. They are requirements for sustained high performance.
The Three-Step Protocol for Managing Impostor Syndrome in Real Time

When the impostor narrative activates before or during a high-stakes professional situation, this protocol interrupts the cycle without requiring extended reflection or processing time.
Step 1: Name the State, Not the Story
The physiological experience of impostor syndrome — elevated heart rate, mental noise, the "I don't belong here" sensation — is a threat response. Name it as such: "My threat system is activated because this matters to me." Do not engage with the content of the narrative. The narrative is generated by the threat state, not by an accurate assessment of your competence. Engaging with it gives it credibility it does not deserve.
Step 2: Apply One Piece of Evidence
Retrieve one specific, factual data point from your Evidence File — or from memory if you do not have a file yet. One concrete example of demonstrated competence in a comparable situation. Not a general reassurance. A specific fact. "I have done this before, in this context, with this outcome." This is not positive thinking. It is accurate data collection.
Step 3: Redirect to the Preparation Question
Replace the question "am I good enough for this?" with "what do I need to prepare, know, or do to perform well here?" This is the only question the situation actually requires an answer to. The impostor question has no productive answer. The preparation question always does. [INTERNAL LINK: Strategic Negotiation Scripts for Women — using preparation to replace anxiety with clarity]
Frequently Asked Questions: Impostor Syndrome at Work
Does impostor syndrome get better with more experience?
Not automatically. Without addressing the asymmetric processing at the root of the cycle, more experience simply provides more high-stakes contexts in which the syndrome activates. The Evidence File method and the reframing described above are more reliable interventions than waiting for experience to resolve it.
Is impostor syndrome more common in women?
The original research focused on women, and there is evidence that certain workplace structures amplify impostor syndrome in women specifically — particularly in industries and roles where women remain underrepresented. The experience itself, however, is broadly distributed. The relevant variable is not gender but the gap between perceived and externally attributed competence, which can affect anyone in a high-stakes professional environment.
What is the difference between impostor syndrome and low confidence?
They frequently co-occur but are functionally different. Low confidence is a stable underestimation of general ability. Impostor syndrome is a specific pattern in which external success is systematically discounted while internal doubt is maintained. Someone with impostor syndrome may present with high confidence in professional contexts while privately believing their success is undeserved. Addressing one does not necessarily address the other.
Can impostor syndrome be useful?
At moderate levels, yes. The self-monitoring and preparation behaviors it produces can improve performance outcomes. The problem arises when the intensity of the response becomes disproportionate to the actual risk, generates avoidance behavior, or connects to burnout through overwork. The goal is calibration, not elimination.
What should I do if impostor syndrome is affecting my ability to ask for a raise or promotion?
The impostor narrative specifically undermines self-advocacy because it frames the ask as something that will "expose" you. The preparation framework is the most effective counter: if you have documented evidence, a clear request, and a value-based rationale, the ask is no longer dependent on how you feel about yourself. It is dependent on the facts.
What Impostor Syndrome Is Actually Telling You
Every working woman who has built something real has felt this. The senior executive who still rehearses presentations twice. The founder who assumes the next thing she attempts will be the one that exposes her. The high performer who reads the same piece of positive feedback five times and still does not quite believe it.
This is not a character flaw. It is not a sign that something is wrong with your psychology. It is a predictable feature of ambitious professional development, and it does not go away by pretending it is not there.
What changes is your relationship to it. When you can look at the self-doubt and recognize it as a signal that you are operating at the edge of your capability, in territory that matters to you, with standards high enough to make the outcome feel consequential, it stops functioning as a verdict. It starts functioning as information.
That is not a small shift. It is the difference between being managed by impostor syndrome and managing it.
Disclaimer: This article provides general psychological information for educational purposes. It does not constitute clinical advice or a substitute for professional psychological support.





